| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
DAFTAR MEMBER ORIFLAME

CEPAT DAN GA RIBET !
Tampilkan postingan dengan label PARASIT. Tampilkan semua postingan
Tampilkan postingan dengan label PARASIT. Tampilkan semua postingan
Kamis, 24 Mei 2012
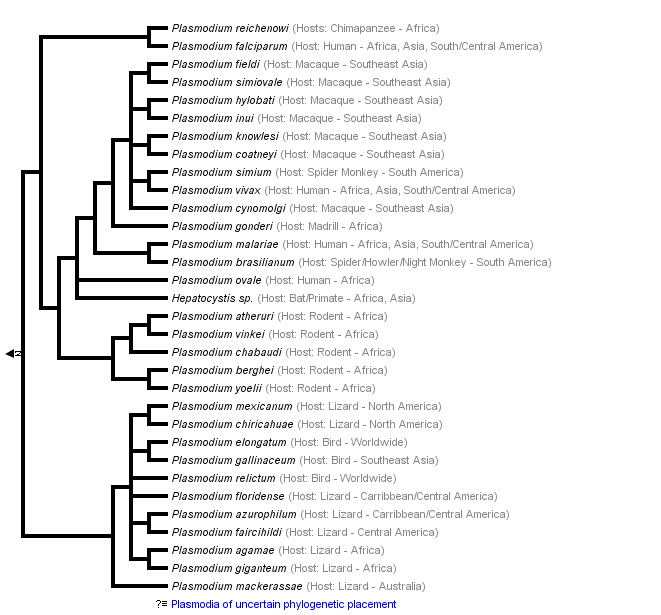
The Malaria Parasites






Selasa, 22 Mei 2012
Elephantiasis
Definition
The word elephantiasis is a vivid and accurate term for the syndrome it describes: the gross (visible) enlargement of the arms, legs, or genitals to elephantoid size.
Description
True elephantiasis is the result of a parasitic infection caused by three specific kinds of round worms. The long, threadlike worms block the body's lymphatic system—a network of channels, lymph nodes, and organs that helps maintain proper fluid levels in the body by draining lymph from tissues into the bloodstream. This blockage causes fluids to collect in the tissues, which can lead to great swelling, called "lymphedema." Limbs can swell so enormously that they resemble an elephant's foreleg in size, texture, and color. This is the severely disfiguring and disabling condition of elephantiasis.
There are a few different causes of elephantiasis, but the agents responsible for most of the elephantiasis in the world are filarial worms: white, slender round worms found in most tropical and subtropical places. They are transmitted by particular kinds (species) of mosquitoes, that is, bloodsucking insects. Infection with these worms is called "lymphatic filariasis" and over a long period of time can cause elephantiasis.
Lymphatic filariasis is a disease of underdeveloped regions found in South America, Central Africa, Asia, the Pacific Islands, and the Caribbean. It is a disease that has been present for centuries, as ancient Persian and Indian writings clearly described elephant-like swellings of the arms, legs, and genitals. It is estimated that 120 million people in the world have lymphatic filariasis. The disease appears to be spreading, in spite of decades of research in this area.
Other terms for elephantiasis are Barbados leg, elephant leg, morbus herculeus, mal de Cayenne, and myelolymphangioma.
Other situations that can lead to elephantiasis are:
- a protozoan disease called leishmaniasis
- a repeated streptococcal infection
- the surgical removal of lymph nodes (usually to prevent the spread of cancer)
- a hereditary birth defect
Causes and symptoms
Three kinds of round worms cause elephantiasis filariasis: Wuchereria bancrofti, Brugia malayi, and Brugia timori. Of these three, W. bancrofti makes up about 90% of the cases. Man is the only known host of W. bancrofti.
Culex, Aedes, and Anopheles mosquitoes are the carriers of W. bancrofti. Anopheles and Mansonia mosquitoes are the carriers of B. malayi. In addition, Anopheles mosquitoes are the carriers of B. timori.
Infected female mosquitoes take a blood meal from a human, and in doing so, introduce larval forms of the particular parasite they carry to the person. These larvae migrate toward a lymphatic channel, then travel to various places within the lymphatic system, usually positioning themselves in or near lymph nodes throughout the body. During this time, they mature into more developed larvae and eventually into adult worms. Depending upon the species of round worm, this development can take a few months or more than a year. The adult worms grow to about 1 in (2.5 cm) to 4 in (10 cm) long.
The adult worms can live from about three to eight years. Some have been known to live to 20 years, and in one case 40 years. The adult worms begin reproducing numerous live embryos, called microfilariae. The microfilariae travel to the bloodstream, where they can be ingested by a mosquito when it takes a blood meal from the infected person. If they are not ingested by a mosquito, the microfilariae die within about 12 months. If they are ingested by a mosquito, they continue to mature. They are totally dependent on their specific species of mosquito to develop further. The cycle continues when the mosquito takes another blood meal.
Most of the symptoms an infected person experiences are due to the blockage of the lymphatic system by the adult worms and due to the substances (excretions and secretions) produced by the worms.
The body's allergic reactions may include repeated episodes of fever, shaking chills, sweating, headaches, vomiting, and pain. Enlarged lymph nodes, swelling of the affected area, skin ulcers, bone and joint pain, tiredness, and red streaks along the arm or leg also may occur. Abscesses can form in lymph nodes or in the lymphatic vessels. They may appear at the surface of the skin as well.
Long-term infection with lymphatic filariasis can lead to lymphedema, hydrocele (a buildup of fluid in any saclike cavity or duct) in the scrotum, and elephantiasis of the legs, scrotum, arms, penis, breasts, and vulvae. The most common site of elephantiasis is the leg. It typically begins in the ankle and progresses to the foot and leg. At first the swollen leg may feel soft to the touch but eventually becomes hard and thick. The skin may appear darkened or warty and may even crack, allowing bacteria to infect the leg and complicate the disease. The microfilariae usually don't cause injury. In some instances, they cause "eosinophilia," an increased number of eosinophils (a type of white blood cells) in the blood.
This disease is more intense in people who never have been exposed to lymphatic filariasis than it is in the native people of tropical areas where the disease occurs. This is because many of the native people often are immunologically tolerant.
Diagnosis
The only sure way to diagnose lymphatic filariasis is by detecting the parasite itself, either the adult worms or the microfilariae.
Microscopic examination of the person's blood may reveal microfilariae. But many times, people who have been infected for a long time do not have microfilariae in their bloodstream. The absence of them, therefore, does not mean necessarily that the person is not infected. In these cases, examining the urine or hydrocele fluid or performing other clinical tests is necessary.
Collecting blood from the individual for microscopic examination should be done during the night when the microfilariae are more numerous in the bloodstream. (Interestingly, this is when mosquitoes bite most frequently.) During the day microfilariae migrate to deeper blood vessels in the body, especially in the lung. If it is decided to perform the blood test during the day, the infected individual may be given a "provocative" dose of medication to provoke the microfilariae to enter the bloodstream. Blood then can be collected an hour later for examination.
Detecting the adult worms can be difficult because they are deep within the lymphatic system and difficult to get to. Biopsies usually are not performed because they usually don't reveal much information.
Treatment
The drug of choice in treating lymphatic filariasis is diethylcarbamazine (DEC). The trade name in the United States is Hetrazan.
The treatment schedule is typically 2 mg/kg per day, three times a day, for three weeks. The drug is taken in tablet form.
DEC kills the microfilariae quickly and injures or kills the adult worms slowly, if at all. If all the adult worms are not killed, remaining paired males and females may continue to produce more larvae. Therefore, several courses of DEC treatment over a long time period may be necessary to rid the individual of the parasites.
DEC has been shown to reduce the size of enlarged lymph nodes and, when taken long-term, to reduce elephantiasis. In India, DEC has been given in the form of a medicated salt, which helps prevent spread of the disease.
The side effects of DEC almost all are due to the body's natural allergic reactions to the dying parasites rather than to the DEC itself. For this reason, DEC must be given carefully to reduce the danger to the individual. Side effects may include fever, chills, headache, dizziness, nausea and vomiting, itching, and joint pain. These side effects usually occur within the first few days of treatment. These side effects usually subside as the individual continues taking the drug.
There is an alternate treatment plan for the use of DEC. This plan is designed to kill the parasites slowly (to reduce allergic reactions to the dead microfilariae and dying adult worms within the body). Lower doses of DEC are taken for the first few days, followed by the higher dose of 2 mg/kg per day for the remaining three weeks. In addition, steroids may be prescribed to prevent the individual's body from reacting severely to the dead worms.
Another drug used is Ivermectin. Early research studies of Ivermectin show that it is excellent in killing microfilariae, but the effects of this drug on the adult worms are still being investigated. It is probable that patients will need to continue using DEC to kill the adult worms. Mild side effects of Ivermectin include headache, fever, and myalgia.
Other means of managing lymphatic filariasis are pressure bandages to wrap the swollen limb and elastic stockings to help reduce the pressure. Exercising and elevating a bandaged limb also can help reduce its size.
Surgery can be performed to reduce elephantiasis by removing excess fatty and fibrous tissue, draining the swelled area, and removing the dead worms.
Prognosis
With DEC treatment, the prognosis is good for early and mild cases of lymphatic filariasis. The prognosis is poor, however, for heavy parasitic infestations.
Prevention
The two main ways to control this disease are to take DEC preventively, which has shown to be effective, and to reduce the number of carrier insects in a particular area.
Avoiding mosquito bites with insecticides and insect repellents is helpful, as is wearing protective clothing and using bed netting.
Much effort has been made in cleaning the breeding sites (stagnant water) of mosquitoes near people's homes in areas where filariasis is found.
Before visiting countries where lymphatic filariasis is found, it would be wise to consult a travel physician to learn about current preventative measures.
Resources
Organizations
National Lymphedema Network. 2211 Post St., Suite 404, San Francisco, CA 94115. (800) 541-3259. 〈http:// www.hooked.net〉.
National Organization for Rare Disorders. PO Box 8923, New Fairfield, CT 06812-8923. (800) 999-6673.http://www.rarediseases.org.
Key terms
Antigen — Any substance (usually a protein) that causes an immune response by the body to produce antibodies.
Filarial — Threadlike. The word "filament" is formed from the same root word.
Host — A person or animal in which a parasite lives, is nourished, grows, and reproduces.
Lymph — A watery substance that collects in the tissues and organs of the body and eventually drains into the bloodstream.
Lymphatic system — A network composed of vessels, lymph nodes, the tonsils, the thymus gland, and the spleen. It is responsible for transporting fluid and nutrients to the bloodstream and for maturing certain blood cells that are part of the body's immune system.
Lymphedema — The unnatural accumulation of lymph in the tissues of the body, which results in swelling in that area.
Protozoa — (Plural form of protozoan) Single-celled organisms (not bacteria) of which about 30 kinds cause disease in humans.
Streptococcal — Pertaining to any of the Streptococcus bacteria. These organisms can cause pneumonia, skin infections, and many other diseases.
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
Lymphatic filariasis
Key facts
- More than 1.3 billion people in 72 countries worldwide are threatened by lymphatic filariasis, commonly known as elephantiasis.
- Over 120 million people are currently infected, with about 40 million disfigured and incapacitated by the disease.
- Lymphatic filariasis can result in an altered lymphatic system and the abnormal enlargement of body parts, causing pain and severe disability.
- Acute episodes of local inflammation involving the skin, lymph nodes and lymphatic vessels often accompany chronic lymphoedema.
- To interrupt transmission WHO recommends an annual mass drug administration of single doses of two medicines to all eligible people in endemic areas.
The disease
Lymphatic filariasis, commonly known as elephantiasis, is a neglected tropical disease. Infection occurs when filarial parasites are transmitted to humans through mosquitoes. When a mosquito with infective stage larvae bites a person, the parasites are deposited on the person's skin from where they enter the body. The larvae then migrate to the lymphatic vessels where they develop into adult worms in the human lymphatic system.
Infection is usually acquired in childhood, but the painful and profoundly disfiguring visible manifestations of the disease occur later in life. Whereas acute episodes of the disease cause temporary disability, lymphatic filariasis leads to permanent disability.
Currently, more than 1.3 billion people in 72 countries are at risk. Approximately 65% of those infected live in the WHO South-East Asia Region, 30% in the African Region, and the remainder in other tropical areas.
Lymphatic filariasis afflicts over 25 million men with genital disease and over 15 million people with lymphoedema. Since the prevalence and intensity of infection are linked to poverty, its elimination can contribute to achieving the United Nations Millennium Development Goals.
Cause and transmission
Lymphatic filariasis is caused by infection with nematodes (roundworms) of the family Filariodidea. There are three types of these thread-like filarial worms:
- Wuchereria bancrofti, which is responsible for 90% of the cases
- Brugia malayi, which causes most of the remainder of the cases
- B. timori, which also causes the diseases.
Adult worms lodge in the lymphatic system and disrupt the immune system. They live for 6-8 years and, during their life time, produce millions of microfilariae (small larvae) that circulate in the blood.
Lymphatic filariasis is transmitted by different types of mosquitoes for example by the Culex mosquito, widespread across urban and semi-urban areas; Anophelesmainly in rural areas, and Aedes, mainly in endemic islands in the Pacific.
Symptoms
Lymphatic filariasis infection involves asymptomatic, acute, and chronic conditions. The majority of infections are asymptomatic, showing no external signs of infection. These asymptomatic infections still cause damage to the lymphatic system and the kidneys as well as alter the body's immune system.
Acute episodes of local inflammation involving skin, lymph nodes and lymphatic vessels often accompany the chronic lymphoedema or elephantiasis. Some of these episodes are caused by the body's immune response to the parasite. However most are the result of bacterial skin infection where normal defences have been partially lost due to underlying lymphatic damage.
When lymphatic filariasis develops into chronic conditions, it leads to lymphoedema (tissue swelling) or elephantiasis (skin/tissue thickening) of limbs and hydrocele (fluid accumulation). Involvement of breasts and genital organs is common.
Such body deformities lead to social stigma, as well as financial hardship from loss of income and increased medical expenses. The socioeconomic burdens of isolation and poverty are immense.
Treatment and prevention
The recommended regimen for treatment through mass drug administration (MDA) is a single dose of two medicines given together - albendazole (400 mg) plus either ivermectin (150-200 mcg/kg) in areas where onchocerciasis (river blindness) is also endemic or diethylcarbamazine citrate (DEC) (6 mg/kg) in areas where onchocerciasis is not endemic. These medicines clear microfilariae from the bloodstream and kill most of the adult worms.
Mosquito control is another measure that can be used to suppress transmission. Measures such as insecticide-treated nets or indoor residual spraying may help protect populations in endemic regions from infection.
Patients with chronic disabilities like elephantiasis, lymphoedema, or hydrocele are advised to maintain rigorous hygiene and take necessary precautions to prevent secondary infection and aggravation of the disease condition.
WHO's response
World Health Assembly Resolution 50.29 encourages Member States to eliminate lymphatic filariasis as a public-health problem.
In response, WHO launched its Global Programme to Eliminate Lymphatic Filariasis (GPELF) in 2000. The goal of the GPELF is to eliminate lymphatic filariasis as a public-health problem by 2020.
The strategy is based on two key components:
- interrupting transmission through annual large-scale treatment programmes, known as mass drug administration, implemented to cover the entire at-risk population;
- alleviating the suffering caused by lymphatic filariasis through morbidity management and disability prevention.
Mass drug administration (MDA)
To achieve interruption of transmission first the disease is mapped to know where to administer MDA then community-wide annual MDA of single doses of albendazole plus either diethylcarbamazine or ivermectin is implemented in endemic regions, treating the entire at-risk population.
MDA should be continued for 4-6 years to fully interrupt transmission of infection. By 2010, 59 endemic countries had completed mapping, and 53 countries had started implementing MDA. Of the 53 countries that had implemented MDA, 37 had already completed five or more rounds of MDA in at least some of their endemic areas.
From 2000 to 2010, more than 3.4 billion treatments were delivered to a targeted population of about 900 million individuals in 53 countries, considerably reducing transmission in many places. Recent research data show that the transmission of lymphatic filariasis in at-risk populations has dropped by 43% since the beginning of the GPELF. The overall economic benefit of the programme during 2000-2007 is conservatively estimated at US$ 24 billion.
Morbidity management
Morbidity management and disability prevention are vital for public health improvement and should be fully integrated into the health system. The GPELF focuses on training health-care workers and communities to dispense proper care and treatment.
Clinical severity of lymphoedema and acute inflammatory episodes can be improved using simple measures of hygiene, skin care, exercise, and elevation of affected limbs. Hydrocele (fluid accumulation) can be cured with surgery.
Kamis, 17 Mei 2012
PROTOZOA
Merupakan filum hewan bersel satu yang dapat melakukan reproduksi seksual (generatif) maupun aseksual (vegetatif).Habitat hidupnya adalah tempat yang basah atau berair. Jika kondisi lingkungan tempat hidupnya tidak menguntungkanmaka protozoa akan membentuk membran tebal dan kuat yang disebut Kista. Ilmuwan yang pertama kali mempelajariprotozoa adalah Anthony van Leeuwenhoek.
PROTOZOA DIBAGI MENJADI 4 KELAS Þ BERDASAR ALAT GERAK
| 1 | Rhizopoda (Sarcodina),alat geraknya berupa pseudopoda (kaki semu) • Amoeba proteus • Entamoeba histolityca • Entamoeba gingivalis • Radiolaria sp. |
| 2 | Flagellata (Mastigophora), alat geraknya berupa nagel (bulu cambuk). Dibagi menjadi 2 kelompok, yaitu: • Golongan phytonagellata - Euglena viridis (makhluk hidup peralihah antara protozoa - Volvax globator (makhluh hidup peralihah antara - Noctiluca millaris (hidup di laut dan dapat mengeluarkan • Golongan Zooflagellata, contohnya : - Trypanosoma gambiense & Trypanosoma rhodesiense. - Trypanosoma cruzl Þ penyakit chagas - Trypanosoma evansi Þ penyakit surra, pada hewan ternak - Leishmaniadonovani Þ penyakit kalanzar - Trichomonas vaginalis Þ penyakit keputihan |
| 3 | Ciliata (Ciliophora), alat gerak berupa silia (rambut getar) • Paramaecium caudatum Þ disebut binatang sandal, yang memiliki dua jenis vakuola yaitu vakuola makanan dan vakuola kontraktil yang berfungsi untuk mengatur kesetimbangan tekanan osmosis (osmoregulator). Memiliki dua jenis inti Þ Makronukleus dan Mikronukleus (inti reproduktif). Cara reproduksi, aseksual Þ membelah diri, seksualÞ konyugasi. • Balantidium coli Þ menyebabkan penyakit diare. |
| 4 | Sporozoa, adalah protozoa yang tidak memiliki alat gerak Cara bergerak hewan ini dengan cara mengubah kedudukan tubuhnya. Pembiakan secara vegetatif (aseksual) disebut juga Skizogoni dan secara generatif (seksual) disebut Sporogoni. Marga yang berhubungan dengan kesehatan manusia ÞToxopinsma dan Plasmodium. Jenis-jenisnya antara lain: - Plasmodiumfalciparum Þ malaria tropika Þ sporulasi tiap hari - Plasmodium vivax Þ malaria tertiana Þ sporulasi tiap hari ke-3 - Plasmodium malariae Þ malaria knartana Þ sporulasi tiap hari - Plasmodiumovale Þ malaria ovale |
Siklus hidup Plasmodium mengalami metagenesis terjadi di dalam tubuh manusia (reproduksi vegetatif Þ skizogoni) dan didalam tubuh nyamuk Anopheles sp. (reproduksi generatif Þ sporogoni). secara lengkap sebagai berikut:
Sporozoit Þ Masuk Tubuh Di Dalam Hati (Ekstra Eritrositer) ÞTropozoid Þ Merozoit (memakan eritrosit Þ Eritrositer) Þ Eritrosit Pecah (peristiwanya Þ Sporulasi) Þ Gametosit Þ Terhisap NyamukÞ Zygot Ookinet Þ Oosis Þ Sporozeit.
Pemberantasan malaria dapat dilakulcan dengan cara :
Sporozoit Þ Masuk Tubuh Di Dalam Hati (Ekstra Eritrositer) ÞTropozoid Þ Merozoit (memakan eritrosit Þ Eritrositer) Þ Eritrosit Pecah (peristiwanya Þ Sporulasi) Þ Gametosit Þ Terhisap NyamukÞ Zygot Ookinet Þ Oosis Þ Sporozeit.
Pemberantasan malaria dapat dilakulcan dengan cara :
- Menghindari gigitan nyamuk Anopheles sp.
- Mengendalikan populasi nyamuk Anopheles dengan insektisidadan larvasida
- Pengobatan penderita secara teratur dengan antimalaria Þchloroquin, fansidar, dll
Rabu, 16 Mei 2012
Entamoeba Histolytica (Amoebiasis)
Entamoeba histolytica is a protozoan parasite responsible for a disease called amoebiasis. It occurs usually in the large intestine and causes internal inflammation as its name suggests (histo = tissue, lytic = destroying). 50 million people are infected worldwide, mostly in tropical countries in areas of poor sanitation. In industrialized countries most of the infected patients are immigrants, institutionalized people and those who have recently visited developing countries.
Inside humans Entamoeba histolytica lives and multiplies as a trophozoite. Trophozoites are oblong and about 15–20 µm in length. In order to infect other humans they encyst and exit the body. The life cycle of Entamoeba histolytica does not require any intermediate host. Mature cysts (spherical, 12–15 µm in diameter) are passed in the feces of an infected human. Another human can get infected by ingesting them in fecally contaminated water, food or hands. If the cysts survive the acidic stomach, they transform back into trophozoites in the small intestine. Trophozoites migrate to the large intestine where they live and multiply by binary fission. Both cysts and trophozoites are sometimes present in the feces. Cysts are usually found in firm stool, whereas trophozoites are found in loose stool. Only cysts can survive longer periods (up to many weeks outside the host) and infect other humans. If trophozoites are ingested, they are killed by the gastric acid of the stomach. Occasionally trophozoites might be transmitted during sexual intercourse.

Most Entamoeba histolytica infections are asymptomatic and trophozoites remain in the intestinal lumen feeding on surrounding nutrients. About 10–20 % of the infections develop into amoebiasis which causes 70 000 deaths each year. Minor infections(luminal amoebiasis) can cause symptoms that include:
- gas (flatulence)
- intermittent constipation
- loose stools
- stomach ache
- stomach cramping.
Severe infections inflame the mucosa of the large intestine causing amoebic dysentery. The parasites can also penetrate the intestinal wall and travel to organs such as the liver via bloodstream causing extraintestinal amoebiasis. Symptoms of these moresevere infections include:
- anemia
- appendicitis (inflammation of the appendix)
- bloody diarrhea
- fatigue
- fever
- gas (flatulence)
- genital and skin lesions
- intermittent constipation
- liver abscesses (can lead to death, if not treated)
- malnutrition
- painful defecation (passage of the stool)
- peritonitis (inflammation of the peritoneum which is the thin membrane that lines the abdominal wall)
- pleuropulmonary abscesses
- stomach ache
- stomach cramping
- toxic megacolon (dilated colon)
- weight loss.
To prevent spreading the infection to others, one should take care of personal hygiene. Always wash your hands with soap and water after using the toilet and before eating or preparing food. Amoebiasis is common in developing countries. Some good practices, when visiting areas of poor sanitation:
- Wash your hands often.
- Avoid eating raw food.
- Avoid eating raw vegetables or fruit that you did not wash and peel yourself.
- Avoid consuming milk or other dairy products that have not been pasteurized.
- Drink only bottled or boiled water or carbonated (bubbly) drinks in cans or bottles.
Natural water can be made safe by filtering it through an "absolute 1 micron or less" filter and dissolving iodine tablets in the filtered water. "Absolute 1 micron" filters are found in outdoor/camping supply stores. Micron = micrometer = 0.001 mm.
Amoebiasis is diagnosed by your health care provider under a microscope by finding cysts and (rarely trophozoites) from a stool sample. The results are usually said to be negative, if Entamoeba histolytica is not found in three different stool samples. But it still does not necessarily mean that you are not infected because the microscopic parasite is hard to find and it might not be present the particular samples. A blood test might also be available but is only recommended, if your health care provider believes that the infection could have spread to other parts of the body. Trophozoites can be identified under a microscope from biopsy samples taken during colonoscopy or surgery.
Entamoeba histolytica should be differentiated from the non-pathogenic Entamoeba dispar. The two are morphologically identical and differentiation must be based on immunologic or isoenzymatic analysis or molecular methods. They can be distinguished under a microscope, if Entamoeba histolytica has ingested red blood cells. Entamoeba dispar is about 10 times more common. If either one is found, then you are usually treated.
If you are experiencing amoebiasis symptoms, you are treated with two antibiotics. The preferred drugs are metronidazole or tinidazole immediately followed with paromomycin, diloxanide furoate or iodoquinol. Asymptomatic intestinal amoebiasis is treated with paromomycin, diloxanide furoate or iodoquinol.



Selasa, 15 Mei 2012
Amoebiasis Disease
Amoebiasis adalah penyakit infeksi usus besar yang disebabkan oleh parasit komensal usus. Penyakit ini tersebar hampir diseluruh dunia terutama di daerah negara tropis yang sedang berkembang. Umumnya disebabkan karena faktor kepadatan penduduk, higiene individu dan sanitasi lingkungan hidup serta kondisi sosial ekonomi dan kultural yang kurang menunjang perilaku kesehatan.
Kasus amoebiasis masih sering di jumpai, baik di pusat kesehatan masyarakat (puskesmas) maupun dalam praktek kedokteran sehari-hari, tetapi penanganannya kadangkala kurang memadai, sehingga akan terjadi komplikasi (penyulit) yang lebih berbahaya. Maka ada baiknya diketahui tentang kasus amoebiasis agar bisa dilakukan penanganan dan pencegahan yang tepat.
- Kuman Penyebab Amoebiasis.
Entamoeba histolytica merupakan protozoa usus, sering hidup sebagai komensal (apatogen=tidak menimbulkan penyakit) di usus besar manusia. Apabila kondisi tubuh mengizinkan dapat berubah menjadi patogen (membentuk koloni di dinding usus, menembus dinding usus dan menimbulkan peradangan). Siklus hidupnya ada 2 macam yaitu bentuk trofozoit yang dapat bergerak dan bentuk kista yang bisa bertahan. - Jenis Kasus Amoebiasis
Kuman amoeba bisa menginfeksi di dalam usus, menimbulkan kasus Amoebiasis Usus Akut, Amoebiasis Usus Kronis (carrier), atau infeksi di luar usus terutama mengakibatkan penyakit Amoebiasis Hati dan Amoebiasis Paru. - Gejala Klinis Amoebiasis
- Amoebiasis Carrier (cyst passer) : tidak menunjukkan gejala klinis sama sekali, karena amoeba yang berada dalam lumen usus besar, tidak mengadakan invasi ke dinding usus.
- Amoebisis Usus Ringan : timbulnya gejala perlahan-lahan, biasanya mengeluh perut kembung, kadang-kadang nyeri perut ringan seperti kejang. Diare ringan, 4-5 kali sehari, tinja berbau busuk, bercampur darah dan lendir, sedikit nyeri tekan di daerah uluhati.
- Amoebisis Usus Sedang : keluhan dan gejala klinis lebih berat dibandingkan disentri ringan, tetapi masih mampu melakukan aktivitas sehari-hari. Tinja disertai darah dan lendir dengan keluhan perut kram, demam dan lemah badan.
- Amoebiasis Usus Berat : mengalami diare disertai darah yang banyak, lebih dari 15 kali sehari, demam tinggi (40 derajat celcius-40,5 derajat celcius), disertai mual dan anemia.
- Amoebiasis kronik : gejalanya menyerupai disentri amoeba ringan, serangan diare diselingi dengan periode normal atau tanpa gejala. Serangan diare biasanya terjadi karena kelelahan, demam atau makanan yang sukar dicerna.
- Penanganan Penyakit Amoebiasis
Obat amoebisid (pemusnah amoeba) tidak bekerja efektif di semua tempat infeksi, terutama bila diberikan dosis tunggal, sehingga dikombinasikan untuk meningkatkan efektifitas pengobatan. Segera konsultasikan dengan dokter, di pusat pelayanan kesehatan terdekat. - Pencegahan Masalah Amoebiasis
Makanan dan air minum sebaiknya di masak dulu dengan baik, karena kista akan binasa bila dipanaskan 50 derajat Celcius selama 5 menit. Penting sekali adanya jamban keluarga, isolasi dan pengobatan terhadap carrier. Khusus untuk seorang carrier (pembawa kista penyakit) dilarang bekerja sebagai juru masak atau segala pekerjaan yang berhubungan dengan makanan.
Demikian pemaparan ringkas kasus amoebiasis, dari berbagai sumber referensi kesehatan. Semoga dapat bermanfaat sebagai perbandingan informasi kesehatan.
Langganan:
Postingan (Atom)